01 — Dissolution Planner
Compile the filler history. Get a per-region plan.
For injectors and patients alike. Add every filler product, volume, and region — the planner returns the anticipated hyaluronidase dose, vials, and draw-up per area. Patients can print or save the record as a PDF to bring to their dissolver.
Anatomic reference
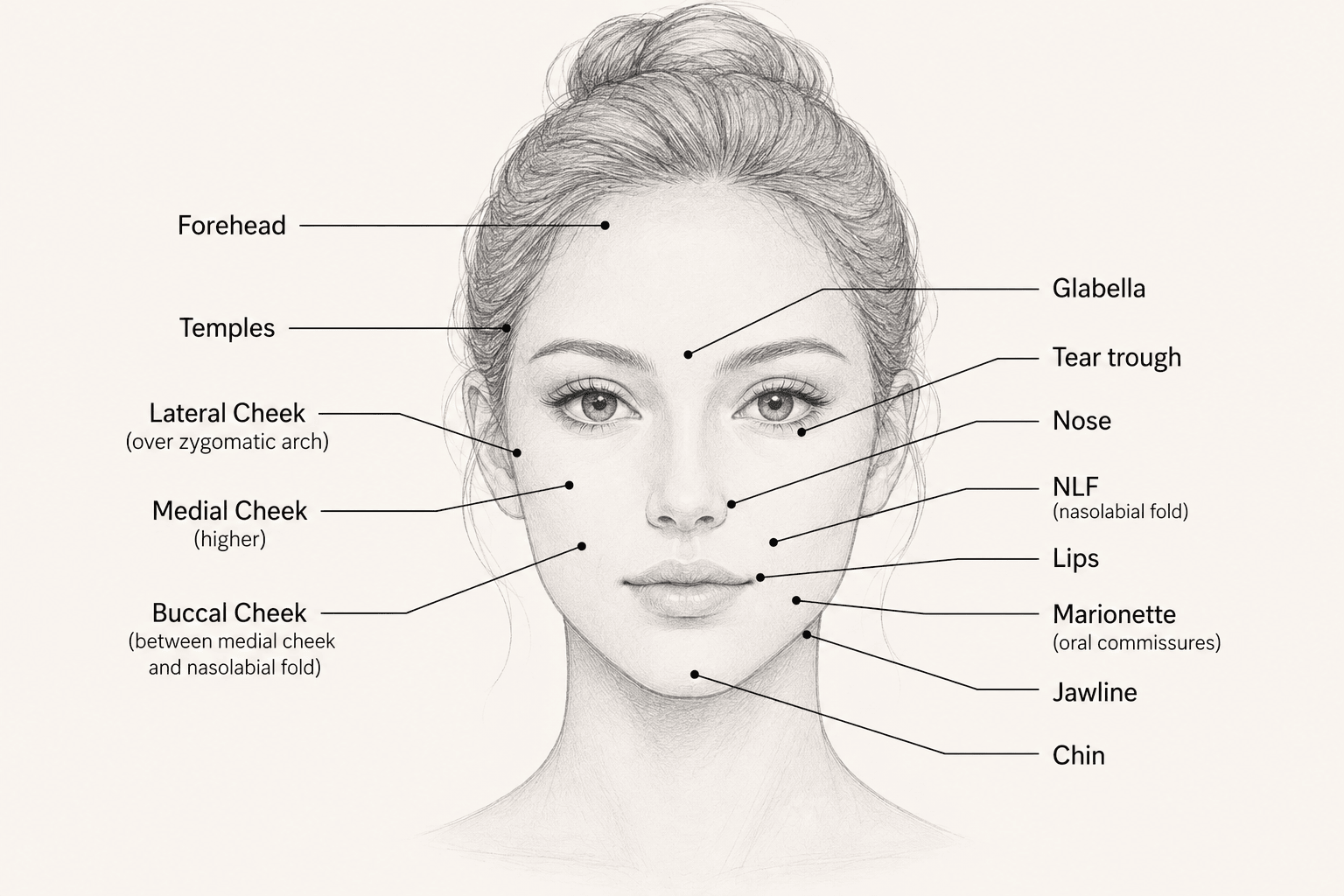
Click image to enlarge. Use the quick-pick or filler dropdown to add entries.
Patient filler history
Dissolution plan — per region
Per-filler baselines pulled directly from the Safran 2025 RHH chart (U recombinant human hyaluronidase / 0.2 mL filler, complete dissolution at one hour, 3:1 dilution; range 2–140 U, ceiling = Belotero Volume at 140 U). Tissue is not a beaker — use the clinical factor below to scale for in-tissue diffusion, chronic filler, high cumulative volume, or known-resistant patient history.
Clinical factor
1.0×
1.0× chart baseline
1.5× standard tissue
2.0× chronic / high-resistance
In vitro chart value — no in-tissue scaling. Use for direct comparison to published Safran 2025 dissolution data.
Add at least one filler entry above to build a dissolution plan.